Radiopharmaceuticals based on novel radionuclides have, for the first time, reached blockbuster proportions. Thierry Stora explains why high-energy physics has an essential role to play in scaling up a life-saving technology.

While radioactivity and radionuclides have been used in medicine for decades, radiopharmaceutical drugs have only recently reached the rank of a pharma blockbuster, with more than one billion US dollars in annual sales. The clearest example is lutetium-177-based therapy, which has moved into routine use for prostate and neuroendocrine cancers, is being investigated as a first-line treatment and generates revenues previously unseen in nuclear medicine (see “How radiopharmaceuticals work” panel).
On the production side, accelerators are a key source of innovation beyond the long-established nuclear reactors. Scaling up these technologies, however, remains challenging. No single laboratory can combine megawatt beams, advanced target engineering and full radiological infrastructure, and the products literally decay on the shelf.
How radiopharmaceuticals work
Modern radiopharmaceuticals combine a radioactive isotope with a biologically active molecule that targets specific cells in the body. The compound is typically injected into the bloodstream, where the biological component guides it to a tumour by binding to a particular protein expressed on cancer cells. Once attached, the radioactive isotope delivers a highly localised dose of radiation that damages or destroys the targeted cells while largely sparing surrounding tissue.
The type of radiation emitted determines how the compound is used. Gamma rays and photons from positron annihilation can escape the body and be detected externally for diagnostic imaging, while Auger electrons, beta particles or alpha particles deposit their energy over very short distances, making them effective for therapy. Increasingly, the same isotope–molecule combination can be used both to image disease and to treat it – an approach known as theranostics.
Many of the technologies now limiting medical radionuclide supply – high-power targets, isotope separation, beam reliability – were originally developed for nuclear and high-energy physics (HEP). These fields will remain essential not because they created today’s tools, but because future medical radionuclide production pushes those tools into regimes that only nuclear physics and HEP routinely explore.
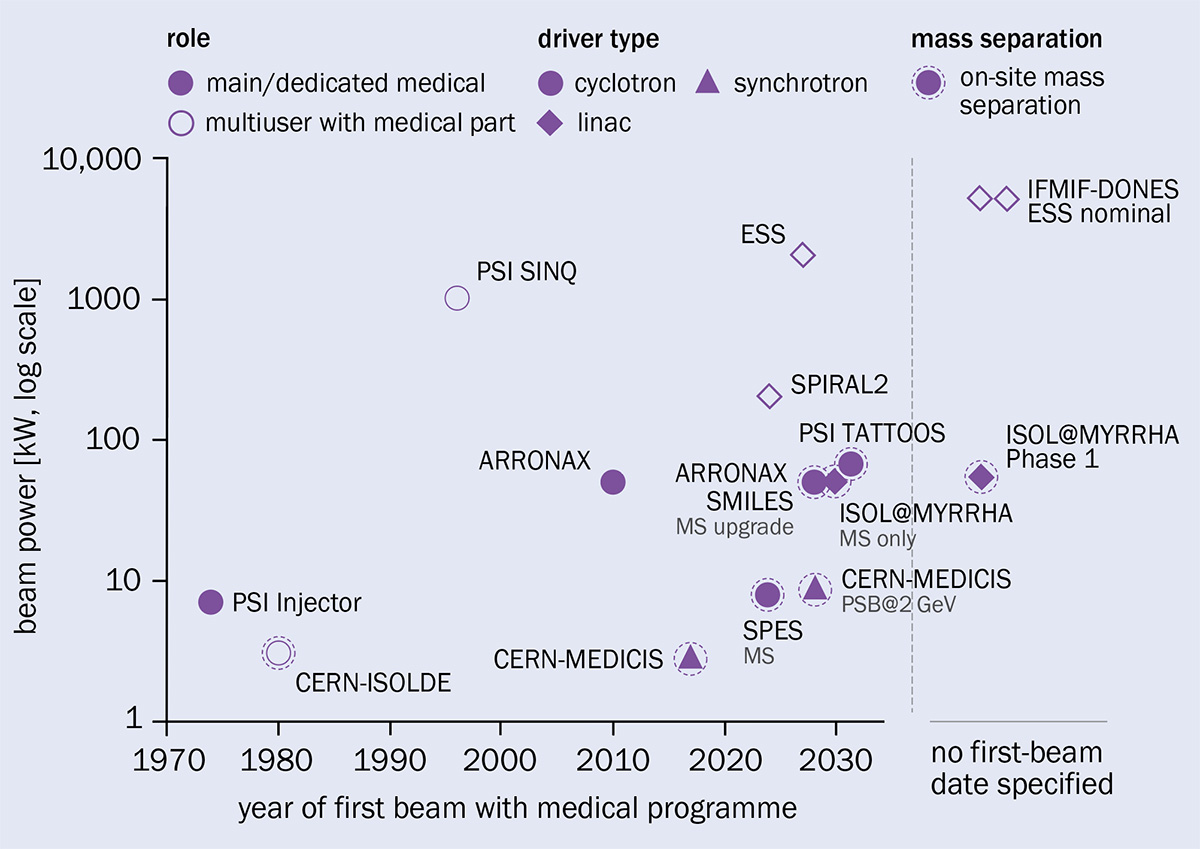
Physicists must address four bottlenecks to meet the growing demand for radiopharmaceuticals, each of which cuts differently across the European accelerator landscape (see “The European landscape” figure). Overcoming these bottlenecks would stabilise the supply of existing treatments and open the door to R&D for entirely new diagnostic and therapeutic isotopes. In that sense, the infrastructure choices made today will shape what kinds of cancer treatments are possible a decade from now.
1. Targets that cannot survive megawatt beams
Large-scale accelerator facilities push beams to extreme power densities in order to generate secondary particles or rare isotopes, placing materials under intense thermal and radiation stress. This regime is familiar from spallation neutron sources, neutrino-production targets and radioactive-ion beam facilities, where target integrity and remote handling are central design challenges rather than secondary considerations. As medical radionuclide production scales up, it increasingly operates in this same regime, where target survivability under sustained continuous-wave irradiation becomes the primary limiting factor. Beyond a certain point, targets degrade, deform or fail faster than they can be replaced, turning material endurance, target design and monitoring – rather than accelerator capability – into the dominant constraint on production.
In practice, this challenge unfolds in two forms, depending on whether a single- or a two-stage target is used. In the two-stage configuration, an intense primary beam is first converted into neutrons or photons, and those secondary particles then irradiate production targets from which the desired radionuclides are generated.
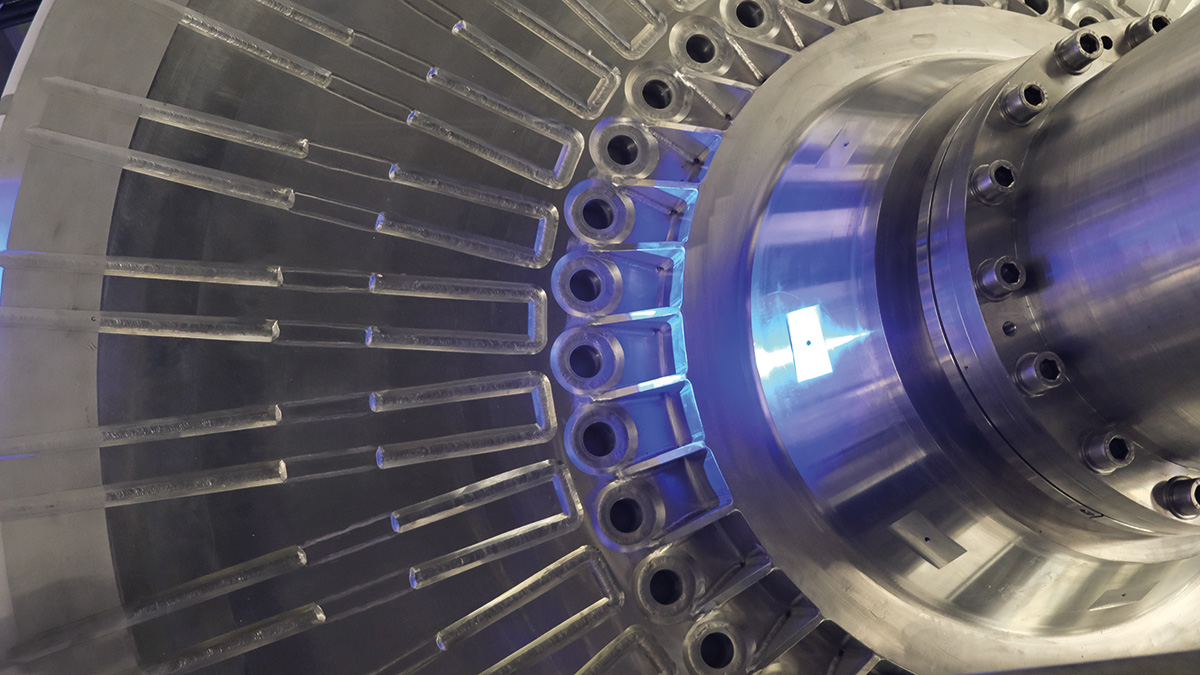
At the very front end of the supply chain, these spallation targets and beam converters – which transform protons into neutrons or electrons into photons – are among the most demanding components in the entire supply chain, because their performance and lifetime cannot be decoupled from beam power. A prominent example is the European Spallation Source (ESS) in Lund, Sweden, which will soon operate the world’s most intense long-pulse neutron beams, where a rotating, helium-cooled tungsten target enables sustained high-power operation (see “Under the beam” image). The pulsed regime introduces additional challenges from shock waves and material fatigue, which must be addressed to ensure safe operations. Likewise, the IFMIF-DONES facility in Granada will combine a 5 MW deuteron beam with a fast-flowing liquid lithium target to generate intense fast-neutron fluxes. While their primary missions lie in fundamental, material and multidisciplinary research, the extreme beam powers and neutron fluxes of these facilities also make them potentially capable of supporting radionuclide production as a secondary, but societally important, application.
Similarly, single-stage targets used for radionuclide production must withstand extreme heat loads and power densities, with geometries that depend on the type and energy of the incident particles. Active cooling, using either gases or liquids, is essential to remove heat, and careful optimisation of both beam delivery and target design can translate directly into higher radionuclide production yields.
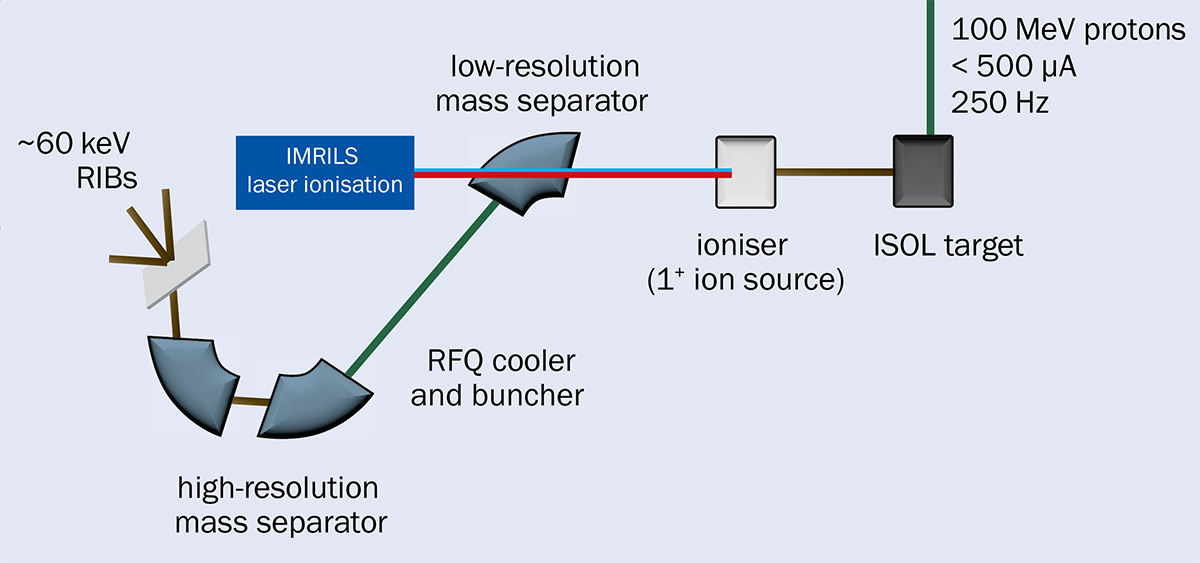
A good example is the development of high-power bismuth targets, in either liquid or solid form, such as those proposed at RIKEN in Japan, which can handle alpha beams of around 10 kW and enable the production of At-211 in batches approaching 100 GBq – far beyond the gigabecquerel-scale batches typical of present-day facilities. RIKEN is Japan’s largest comprehensive research institute, operating major accelerator and nuclear-physics facilities with a long-standing programme in medical radionuclide production. In Europe, comparable facilities are under construction, such as SPIRAL2 in Caen, France, or at SCK CEN in Mol, Belgium, where ISOL@MYRRHA will deliver a 100 MeV proton beam of up to 500 µA onto a target dedicated to the production of medical and research radionuclides (see “Sorting the haul” figure).
Additional challenges arise for highly radioactive targets such as Ra-226, a long-lived precursor used in the production of the alpha-emitting medical isotopes Ac-225 or Ra-224, or for targets designed for high-power operation and mass separation, which must remain structurally and chemically stable at temperatures approaching 2500 °C.
Even when targets survive extreme beam power, increased production immediately creates a second constraint: the radionuclides they produce are only useful if they can be isolated in the required purity – a challenge that defines the next bottleneck.
2. Radionuclides that cannot be separated
When radioactive products are chemically indistinguishable from unwanted isotopes, separation must rely on their mass rather than on their chemical properties. Without such separation, many promising medical radionuclides cannot be used at all, regardless of how efficiently they are produced, because they remain too dilute or come with long-lived impurities. This challenge is familiar from isotope production for nuclear and particle physics, where ion sources, mass separators and laser techniques are used to extract rare species from intense backgrounds.
A dedicated collaborative infrastructure was established at CERN with the creation of CERN-MEDICIS, which received support from the CERN & Society Foundation and pioneers isotope mass separation for medical applications. Commissioned in 2017, MEDICIS brings together expertise in target production, purification, radiopharmaceutical development and clinical use, linking large-scale physics infrastructure directly to biomedical research.
Building on techniques originally developed at ISOLDE, the MEDICIS programme has adapted isotope mass separation specifically for medical needs. This has enabled access to radionuclides that are otherwise unavailable, or available only at insufficient purity, achieving high molar activities essential for theranostic and therapeutic applications.
In contrast to radiochemical separation, which typically achieves efficiencies above 95%, mass-separation efficiencies vary widely, ranging from a few percent to around 70%, depending on the isotope and production route. As a result, scaling up production by mass separation is not a matter of incremental optimisation: gains in yield must be traded against beam power, target lifetime and radiation handling, placing practical limits on what facilities can deliver for many isotopes.
Significant progress has nevertheless been achieved through advances in target design, compact ion sources and resonant laser ionisation, with efficiencies above 50% now considered high performance for these physics-driven separation processes. Operating at higher beam intensities further opens the possibility of separating radionuclides directly from reactor or cyclotron targets, but doing so requires accelerator conditions and radiation handling capabilities that are only available at large-scale research infrastructures. Because mass separation is both technically demanding and intrinsically inefficient, access to purified radionuclides cannot be scaled locally, making coordination across large research infrastructures unavoidable.
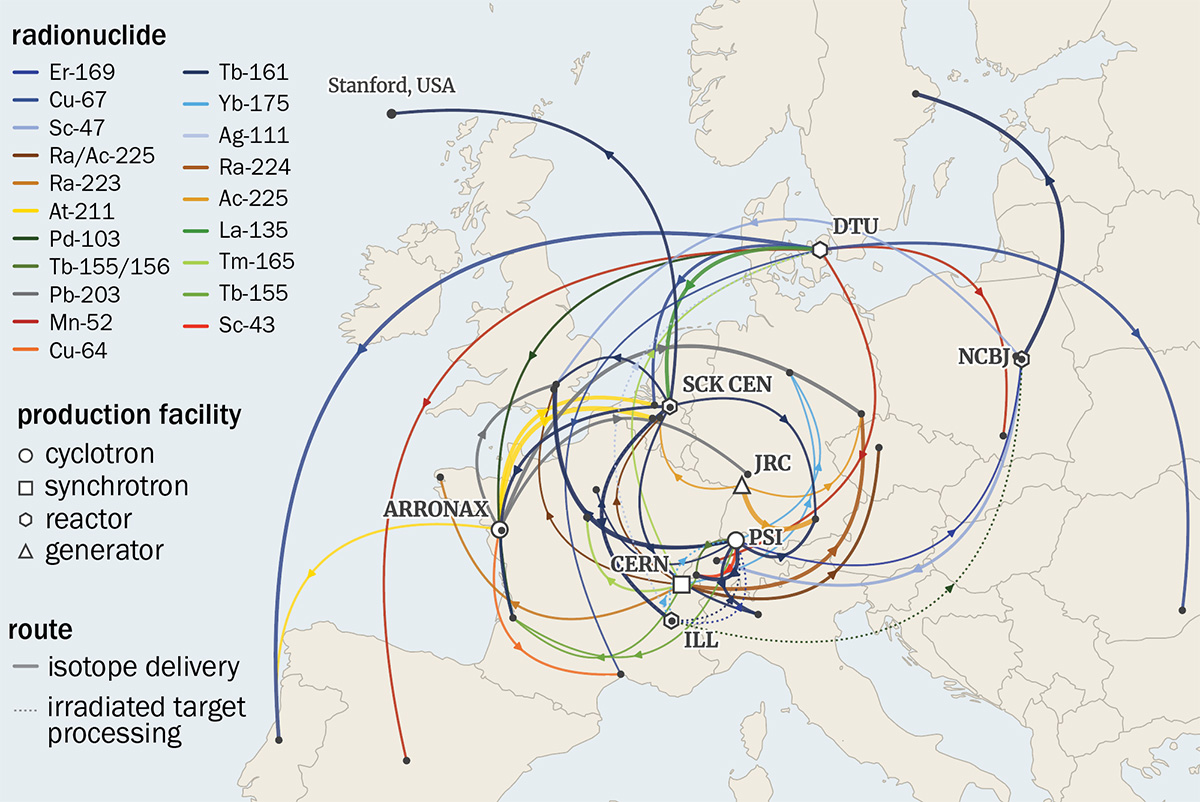
In Europe, this need for coordination has been addressed through a networked approach rather than a single flagship facility. The PRISMAP programme (H2020 grant #101008571), and its follow-up PRISMAP+, bring together accelerators, reactors, isotope separation facilities and biomedical hubs across national borders, allowing researchers to access purified radionuclides that no single site could reliably supply on its own (see “Special delivery” figure). By pooling infrastructure, expertise and scheduling through competitive calls, PRISMAP has lowered the barrier for biomedical researchers to work with non-conventional radionuclides, while preserving the efficiency and safety constraints imposed by large-scale physics infrastructure. It is becoming the European medical radionuclides programme that biomedical research lacked.
The same mismatch between research-scale tools and medical-scale demand reappears in accelerator design itself – the focus of the next bottleneck.
3. Machines optimised for experiments, not production
Accelerators developed for fundamental research are typically optimised for peak performance, flexibility and discovery-driven operation. Medical radionuclide production, by contrast, demands continuous, predictable delivery, exposing a growing mismatch between machines designed for experiments and those required for routine isotope production. In practice, the requirements of medical radionuclide production change dramatically between exploratory research and routine clinical supply, shifting the emphasis from flexibility and peak performance towards reliability, uptime and predictable delivery.
Scaling requires not only new radionuclides, but integrated infrastructures
Improving multi-user operation and reducing maintenance downtime can already deliver substantial gains in effective output, even without higher beam power. Intense beams of light ions and electrons are available today using cyclotrons and linear accelerators, while new concepts are being developed to better match medical needs, including synchrotrons for alpha particles and high-power electron sources for photon-based production routes.
Even when suitable accelerators exist, however, delivering medically usable radionuclides depends on meeting regulatory, dosimetric and logistical constraints that lie beyond the machine itself.
4. Production without regulatory viability
Unlike research isotopes, radiopharmaceuticals must meet strict regulatory, dosimetric and logistical requirements. Even small uncertainties in nuclear data, impurity levels or processing routes can prevent a radionuclide from reaching patients, regardless of its therapeutic promise. At this stage, scale is limited not by beam power or yield, but by whether a radionuclide can be licensed, transported and used safely in the clinic.
The case of lutetium-177 (Lu-177) illustrates both the challenge and the opportunity. Its success has been central to the emergence of modern radiotherapeutic drugs, with compounds targeting prostate and neuroendocrine cancers now used routinely in clinical practice. This success rests not only on biological targeting, but on a carefully controlled production chain that meets pharmaceutical standards.
The mode of production of Lu-177 – either by direct neutron capture on Lu-176 or via an indirect route through Yb-176 – highlights the complexity of aligning nuclear physics, infrastructure and regulation. Choices made upstream determine radionuclidic purity, waste streams and processing requirements downstream, all of which feed directly into licensing and clinical acceptance. Lu-177’s physical and radiological properties, including its suitability for both imaging and therapy, and a half-life of about 6.64 days that is compatible with existing medical logistics, have helped it integrate into an established supply-chain organisation. This combination has enabled treatments to reach large patient populations and commercial scale.
Meeting these requirements demands substantial investment beyond irradiation itself. Facilities must support radiochemical processing, quality control, dosimetry and specialised logistics, often in shielded hot-cell environments. Recent upgrades to such infrastructure have shown that production capacity can increase significantly once these downstream constraints are addressed. At the same time, improved nuclear and biological data have revealed that even modest discrepancies in decay properties or radiation dose can have major consequences for treatment planning, licensing and waste management.
Programmes such as PRISMAP+ have begun to address this bottleneck by providing access to novel treatment radionuclides, including beta emitters that extend established therapies such as Lu-177. By generating data on production quality and radiochemical behaviour early in development, these programmes help determine which radionuclides can realistically progress from research to routine clinical use. Crucially, regulatory constraints feed back into accelerator choice, target design and separation strategy: decisions taken at the level of beam energy, target material and purification method determine whether a radionuclide can ever meet clinical purity, waste and licensing requirements.
Taken together, these constraints show why regulatory viability is itself a bottleneck. Scaling radiopharmaceuticals requires not only new radionuclides, but integrated infrastructures in which production, processing, regulation and clinical deployment are addressed together. As radiopharmaceuticals move further into mainstream oncology, success will depend on sustained collaboration between large-scale research infrastructures, regulators, clinicians and industrial partners – none of which can solve the problem alone.
• The author dedicates this article to the memory of Mark Rayner, who shaped its structure and much of its prose.